

BACKGROUND: The outcome of patients with acute lymphoblastic leukemia (ALL) aged above 55 years treated with conventional-dose chemotherapy is poor. Due to the frequent presence of co-morbidities many patients are ineligible for myeloablative allogeneic (allo) hematopoietic cell transplantation (HCT). The role of autologous (auto) HCT and reduced intensity conditioning (RIC)-alloHCT is not well-established. The goal of this study was to analyze results of these transplant options and to identify factors affecting outcome.
PATIENTS: Five-hundred and sixty patients with ALL treated in first complete remission (CR1) with RIC-alloHCT (n=418) or autoHSCT (n=142), between 2000-2018, were included in the analysis. Among allogeneic donors, 50% were HLA-matched sibling donors (MSD) and 50% were 8/8 HLA matched unrelated donors (MUD). Median age for RIC-alloHCT and autoHCT was 60 (range 55-76) years and 61 (range 55-76) years, respectively. The proportion of Philadelphia chromosome positive (Ph(+)) ALL was 71% and 63%, respectively. Measurable residual disease (MRD)-positive status at the time of HCT was reported in 35% and 21% patients, respectively (p=0.002). Busulphan and fludarabine (BuFlu) was the most frequently used conditioning regimen in the RIC-alloHCT setting (34%) while a combination of 12 Gy total body irradiation/cyclophosphamide (TBI12Gy/Cy) was most frequent in the autoHCT group (33%).
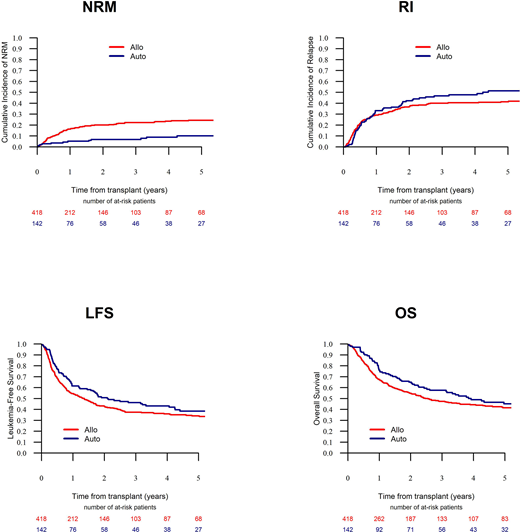
RESULTS: The engraftment rate was 99% after RIC-alloHCT and 96% after autoHCT (p=0.01) while median time to neutrophil recovery was 16 days and 12 days, respectively (p<0.001), respectively. With a median follow-up of 57 months, the probabilities of leukemia-free survival (LFS) and overall survival (OS) at 5 years were 39% versus 34% (p=0.11) and 45% vs. 42% (p=0.23), respectively. The incidence of relapse (RI) and non-relapse mortality (NRM) were 41% vs. 51% (p=0.22) and 25% vs. 10% (p=0.001), respectively. In a multivariate model, using autoHCT as reference, the risk of NRM was increased for MSD-HCT (HR=2.1, p=0.02) and MUD-HCT (HR=3.08, p<0.001), which for MUD-HCT translated into a decreased chance of LFS (HR=1.55, p=0.01) and OS (HR=1.62, p=0.008). For MSD-HCT there was a tendency towards decreased LFS (HR=1.31, p=0.11) and OS (1.29, p=0.15) when compared to autoHCT. Among other prognostic factors, the risk of relapse was decreased for Ph(+) ALL compared to Ph(-) B-ALL (HR=0.7, p=0.04) which was accompanied by improved OS (HR=0.74, p=0.04). Finally, the risk of relapse was increased for patients with detectable MRD (HR=1.38, p=0.04) without significant effect on survival.
CONCLUSIONS: Results of autoHCT for patients with ALL aged above 55 years in CR1 and with MRD negativity pre-transplant are encouraging. This option may be a valuable alternative to RIC-alloHCT and is associated with an improved OS compared to transplantations from MUD. Our observations require verification in prospective trials in the context of currently available novel agents and technologies, including blinatumomab, inotuzumab ozogamicin and CAR-T cells.
Figure. Results of RIC-alloHCT and autoHCT for patients with ALL in CR1 aged >55 years
Labopin:Jazz Pharmaceuticals: Honoraria. Blaise:Jazz Pharmaceuticals: Honoraria. Forcade:Novartis: Other: Travel grant for congress; Sanofi: Other: Travel grant for congress; JAZZ: Other: Travel grant for congress; NEOVII: Other: Travel grant for congress; Gilead: Speakers Bureau. Yakoub-Agha:Janssen: Honoraria; Gilead/Kite: Honoraria, Other: travel support; Novartis: Honoraria; Celgene: Honoraria; Jazz Pharmaceuticals: Honoraria. Mohty:Sanofi: Consultancy, Honoraria, Research Funding, Speakers Bureau; Stemline: Consultancy, Honoraria, Research Funding, Speakers Bureau; Novartis: Consultancy, Honoraria, Research Funding, Speakers Bureau; BMS: Consultancy, Honoraria, Research Funding, Speakers Bureau; Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding, Speakers Bureau; Amgen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau; GSK: Consultancy, Honoraria, Research Funding, Speakers Bureau; Takeda: Consultancy, Honoraria, Research Funding, Speakers Bureau; Celgene: Consultancy, Honoraria, Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal